Prostatic Artery Embolisation
An innovative non-surgical, minimally invasive technique to treat symptoms of benign prostatic hyperplasia. Performed under precise radiological guidance by an expert team.
Looking for answers based on your symptoms?
Read our patient guide: Waking up at night to urinateWhy Prostate Embolisation?
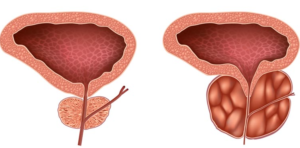
Prostate embolisation is an innovative non-surgical, minimally invasive technique to treat symptoms of benign prostatic hyperplasia (BPH), also known as prostate adenoma.
Prostate enlargement is very common from age 50 onwards. This increase in volume can cause bladder outlet obstruction and irritative urinary symptoms in some patients. Lower urinary tract symptoms significantly affect men's quality of life increasingly after age 50. Although BPH is extremely common (46% in men over 60), associated symptoms are not always related to prostate enlargement. Other causes must be ruled out (bladder, neurological, etc.). Nevertheless, these symptoms (dysuria, pollakiuria, nocturia, etc.) can have a significant impact on quality of life and even sexual function.
Which Patients Are Suitable for Prostate Embolisation?
Embolisation is performed as an alternative to transurethral surgery (transurethral resection of the prostate or more recently laser surgery: HoLEP®, GreenLight®) and to other minimally invasive treatments (UroLift®, Rezum®, Aquabeam®). Treatment criteria for embolisation are currently the same as for surgery (moderate to severe lower urinary tract symptoms, partly based on the IPSS score).
The final therapeutic decision rests with the patient after discussion with the relevant physicians (GP, urologist and interventional radiologist).
It is important to rule out any underlying cancer. Active surveillance of low-grade cancer (Gleason 6) is not an absolute contraindication to embolisation, but these cases must be discussed at multidisciplinary team meetings like any cancer.
There is no upper size limit for embolisation and effects are even enhanced in large prostates. However, below 35 to 40 g the procedure becomes technically difficult and the benefit questionable.
The presence of a median lobe is not an obstacle to embolisation.
Contraindications:
- Renal insufficiency
- Prostate cancer requiring specific curative treatment (radiotherapy or radical prostatectomy)
- Severe unbalanced iodinated contrast allergy
Coagulation workup and prostate volume measurement are essential preliminary steps, as is urological assessment. The procedure can be performed on antiplatelet agents or even anticoagulation depending on the patient (particularly with radial access). PSA testing is also required as part of prostate cancer screening.
How Is Prostate Embolisation Performed?
The procedure is performed on an outpatient basis under local anaesthesia and without bladder catheterisation.
The patient is admitted in the morning and discharged in the late afternoon after urinating, without pain.
The procedure lasts 45 minutes to 1 hour 30 depending on technical difficulty. The more tortuous the vascular anatomy (common in older patients), the more complicated catheterisation may be.
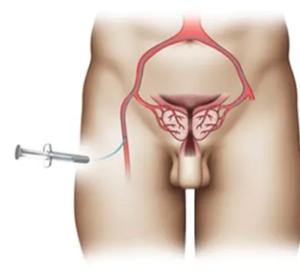
The radiologist establishes arterial vascular access (left radial or right femoral depending on each patient's anatomy) under local anaesthesia and ultrasound guidance.

Radial access is commonly used in interventional cardiology for coronary angiography but is still little used by interventional radiologists. The advantage of the radial route is a lower puncture site complication rate (particularly haematoma) and the ability for the patient to walk immediately after the procedure and leave the day unit more quickly; conversely, the femoral route requires bed rest for at least 4 hours. However, it cannot be used in very tall patients.
Once arterial access is in place, the procedure is completely painless.
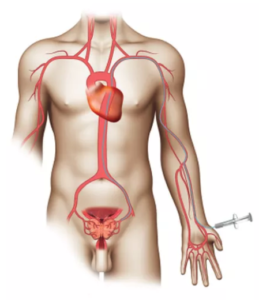
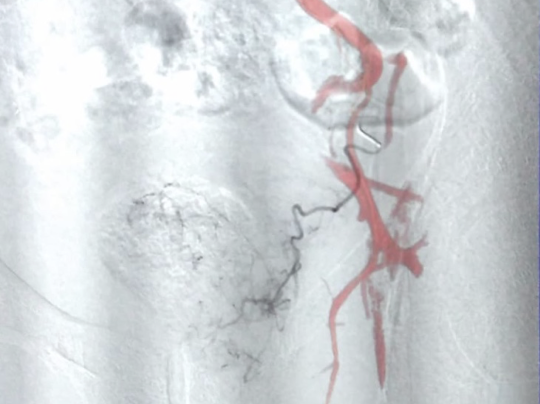
A 1.6 mm catheter is introduced through the arterial access and guided using X-rays to the internal iliac arteries. A 0.6 mm microcatheter is then introduced into the carrier catheter (co-axial system) to reach the prostatic arteries.
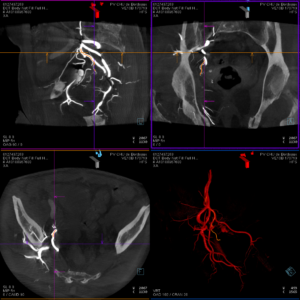
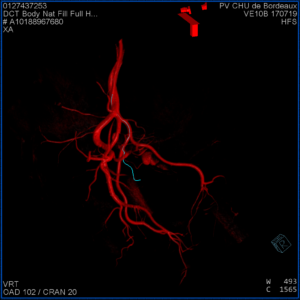
Prostatic arteries have many anatomical variants, which makes the procedure potentially difficult. There may be one to two arteries per side (1.4 on average). Prostatic artery diameter is approximately 1 mm. The origin of these arteries varies greatly between patients. 3D acquisition allows identification of prostatic arteries and catheterisation using fusion of 3D and fluoroscopic images.
Once in the prostatic artery, 3D acquisitions confirm the absence of anastomoses and therefore the absence of off-target embolisation risk. Microparticles (average diameter 300 to 500 microns) are then injected until complete cessation of flow. These may be replaced or supplemented by liquid agents (Onyx® or Glubran®) depending on vascular configuration, with the advantage of complete and definitive occlusion of the target vessel with better visualisation during injection.
EmboGold® Microspheres – Calibrated microparticles for prostatic artery embolisation.

There is no risk of particle migration after embolisation. The particles are "trapped" in the smallest vessel they can reach.
What Happens After Embolisation?
After embolisation, the patient spends a brief period (45 minutes) in the post-procedure room, then returns to the day unit where the interventional radiologist will discharge them in the afternoon.
Post-embolisation syndrome is systematic after prostate embolisation. It is secondary to gland inflammation after vessel occlusion and causes irritative symptoms (pollakiuria, urinary burning, among others) for an average of 3 to 7 days. In rare cases, fever may occur. Bacterial cultures are negative.
The higher the prostate volume, the more marked this syndrome (particularly above 100 g or ml of prostatic tissue). Sometimes post-embolisation syndrome can be very bothersome and last 2 weeks.
The Centre Aquitain d'Imagerie team works closely with the MidiPerf team for home care follow-up, supported by a network of community nurses.
What Are the Side Effects of Prostate Embolisation?
The patient may exceptionally experience haemospermia, haematuria or rectal bleeding, which are not serious. All are transient (approximately 2 weeks).
Potential complications include:
- Puncture site haematoma (less frequent via radial route)
- Prostatitis (infectious) treated with antibiotics: rare and more common in patients with permanent catheters
- Off-target embolisation (exceptional thanks to 3D imaging)
Beneficial effects of the procedure are felt after 15 days to 1 month, with a plateau around 3 months.
Usual urinary medication is continued for 1 month after embolisation.
There is no effect on sexual function. Some studies have even shown improvement in sexual function score (IIEF5).
What Are the Long-Term Effects After Prostate Embolisation?
Effects on lower urinary tract symptoms are durable and follow-up, although limited (20 years), currently shows very good efficacy for an extremely limited risk.
After prostatic artery embolisation, there is never retrograde ejaculation (which is constant after surgery).
Pelvic floor rehabilitation before and after the procedure may enhance the intervention.
In case of embolisation failure (5 to 10% depending on series), a second attempt may be considered.
After clinical failure, another treatment, particularly surgery, is perfectly feasible, especially as some teams have shown the efficacy of an embolisation-then-surgery sequence.
In our experience, surgery after embolisation is a rare option due to the very frequent technical success of the procedure.
The patient can return to work approximately 5 days after embolisation.
Sexual activity is not restricted after the procedure, but due to post-embolisation syndrome, it is generally not appropriate for the first 5 days.
The patient is reviewed in consultation 3 months after embolisation.
How Much Does Prostate Embolisation Cost?
The procedure is reimbursed by the French social security system (Supra-selective embolisation of a branch of the internal iliac artery – EDSF004).
At Bordeaux University Hospital, no fee over and above standard reimbursement is charged. This may vary between centres.
For foreign nationals not covered by social security, the total cost of the procedure at Bordeaux University Hospital is currently less than €1,800 (February 2023, subject to change).
A quote must be provided by the healthcare facility treating the patient.
What Do You Need Before a Consultation with the Radiologist?
- PSA test
- Prostate imaging (ideally MRI)
- Optional: urodynamic assessment, pelvic vessel CT angiography
Explanatory Video
An explanatory video detailing the prostatic artery embolisation procedure is available on YouTube. It illustrates the steps of the procedure, vascular access, catheterisation of prostatic arteries and injection of embolic agents under radiological guidance.
If the video does not load, Prostate Embolisation – Explanatory Video
Which Hospitals and Clinics Perform Prostate Embolisation?
Prostatic artery embolisation is an innovative technique performed in the leading interventional radiology centres in France, Belgium, overseas territories and internationally.
South-West: Clinique Mutualiste de Pessac (Centre Aquitain d'Imagerie), Bordeaux University Hospital, Bayonne, Pau, Toulouse, La Rochelle, Limoges.
Paris and Île-de-France: Saint Louis Hospital, HEGP, American Hospital of Paris, Henri Mondor University Hospital, Tenon, Bichat, Cochin, Paris and suburban clinics.
North and North-East: Valenciennes, Amiens, Rouen, Strasbourg, Nancy.
West: Brest, Poitiers, Rennes, Angers, Nantes, Caen, Le Mans, Vannes.
East and South-East: Lyon, Dijon, Grenoble, Annecy, Marseille, Nice, Toulon, Montpellier, Nîmes, Perpignan.
Central France, overseas territories, Belgium and international: Clermont-Ferrand, Réunion Island, Belgian centres (Brussels, Namur, Tournai), Switzerland (Lausanne), Tunisia, Morocco.
Interactive map of centres performing prostatic artery embolisation (France, Belgium, Switzerland). Click a marker for details.
Also performed in Réunion, Tunisia and Morocco (outside the metropolitan map).
Not listed? Please contact us at: f.petitpierre@lecai.fr
Ready to book an appointment?
Contact us to discuss your situation and schedule your consultation
Book an appointment