Knee Pain Treatment by Radiofrequency
A safe and effective minimally invasive technique to treat knee pain related to osteoarthritis or persisting after prosthesis. Performed under precise radiological guidance by an expert team.
What is the principle of radiofrequency?
This is a technique used in interventional radiology with several applications. Here, the goal is to relieve knee pain.
Pain is sensory information transmitted to the brain via a nerve. Schematically, a nerve can be compared to an electrical cable with wires inside and an outer sheath. Radiofrequency damages the cable sheath, preventing the pain signal from reaching the brain.
At the knee, several nerves called genicular nerves have been identified in the participation of this painful symptomatology.
What are the indications for analgesic radiofrequency?
This technique is indicated in 2 main situations:
- Knee pain secondary to osteoarthritis that resists medication, physiotherapy, and injections (corticosteroids, hyaluronic acid, and PRP). Radiofrequency is then an option, especially if the patient is young and time needs to be gained before possible prosthetic surgery.
- Knee pain persisting after total knee replacement. Scientific literature reports a rate of 20% of total knee replacements (TKR) that remain painful without identified cause.
Does radiofrequency treat osteoarthritis?
No. Radiofrequency treats pain secondary to osteoarthritis, but the main cause, osteoarthritis, continues to progress.
Osteoarthritis is a physiological phenomenon, meaning normal from a certain age depending on several factors (obesity, occupational life, genetics, etc.), and not all osteoarthritis is painful.
Radiofrequency is therefore part of the therapeutic arsenal for pain related to osteoarthritis.
Regarding patients with a knee prosthesis, pain is not always the only symptom. Stiffness may also be present. Analgesic radiofrequency has no effect on knee stiffness. However, if pain is reduced after radiofrequency, it is advisable to start a new course of physiotherapy to combat stiffness and strengthen musculature.
What examinations should be performed before radiofrequency?
It is preferable to have had a prior consultation with your general practitioner or a specialist, as well as imaging workup including X-rays or MRI.
There is then the diagnostic block step, which consists of injecting a dose of anesthetic under guidance along the nerve pathways to temporarily "numb" them. If pain decreases by 50% after the block, the test is considered positive and radiofrequency can be offered.
How is radiofrequency performed?
Radiofrequency is an outpatient procedure with an estimated duration of approximately 30 minutes.
- The patient lies on their back with the knee to be treated in slight flexion. Adhesive pads are placed on the ipsilateral thigh for the procedure.
- The knee is disinfected before starting the procedure with local anesthesia for patient comfort.
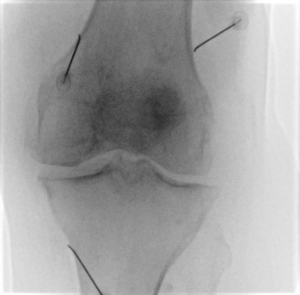
- Radiofrequency needles are placed under guidance. The number of needles varies depending on the procedure and clinical scenario.
- Once in place, a preliminary motor and sensory test is performed to ensure needles are correctly positioned, particularly away from major motor nerves.
- Heating through the needles can then begin and generally lasts 60 seconds per needle.
- The needles are then removed and simple dressings are applied before return to the outpatient unit where the patient is generally kept for 2 hours before discharge home.
Discharge home must be accompanied. A transport voucher can be arranged for isolated patients.
What is the recovery like? Will I be relieved immediately?
Immediate recovery is marked by transient pain along the needle tracts for 24–48 hours.
Return to activities should be gradual from 48 hours onward and during the following week: avoid unusual physical exertion during the first 7 days.
Pain relief generally occurs within 6 weeks following the procedure. This delay must be waited before judging effectiveness.
As a reminder, the goal is a 50% reduction in painful symptoms, which remains subjective. Complete disappearance may occur in some cases but is not the rule.
Is it a permanent treatment?
There is a risk of recurrence because the procedure damages the nerve myelin sheath without completely destroying the nerve. This sheath will regenerate and pain may recur, although this occurs after several months or even a year.
If relief was significant over a long period, the procedure can be repeated.
What are the possible complications?
The risks associated with this procedure are very low but exist, as with all interventions.
Risks common to all procedures:
- Hemorrhagic risk: hematoma along the tract. However, the caliber of needles used is small, minimizing this risk. It is important to report antiplatelet or anticoagulant medication during consultation.
- Infectious risk: also low because there is no skin opening and the procedure is performed in an interventional radiology suite under aseptic conditions.
- Anesthesia-related risks: allergy to products used during anesthesia or decompensation of underlying pathology (cardiovascular, respiratory, etc.).
Risks specific to analgesic radiofrequency:
- Tingling in the legs: related to nerve irritation secondary to the procedure. Most often spontaneously regressive within a few days.
- Motor deficit in the leg: serious theoretical complication related to incorrect needle positioning. This exceptional complication is prevented by the motor test performed once the needle is in place and before heating begins, as well as by precise imaging means to control needle positioning.
Are there contraindications?
The main contraindications to these procedures are related to the presence of the following devices:
- Pacemaker
- Defibrillator
- Neurostimulation device
Pregnancy is of course a contraindication due to the use of X-rays.
What are the alternatives?
In knee osteoarthritis, radiofrequency treatment is a third-line treatment. It is generally indicated after first-line treatment consisting of medication and physiotherapy, and after second-line treatments, namely injections. The last-line treatment for knee osteoarthritis is prosthesis.
In case of pain on prosthesis, it is important to find the cause of pain. This may be septic or aseptic loosening, tendinopathy, fibrosis, etc. A complete workup must therefore be performed, and only when no cause is identified is analgesic radiofrequency considered.
Ready to book an appointment?
Contact us to discuss your situation and schedule your consultation
Book an appointment